
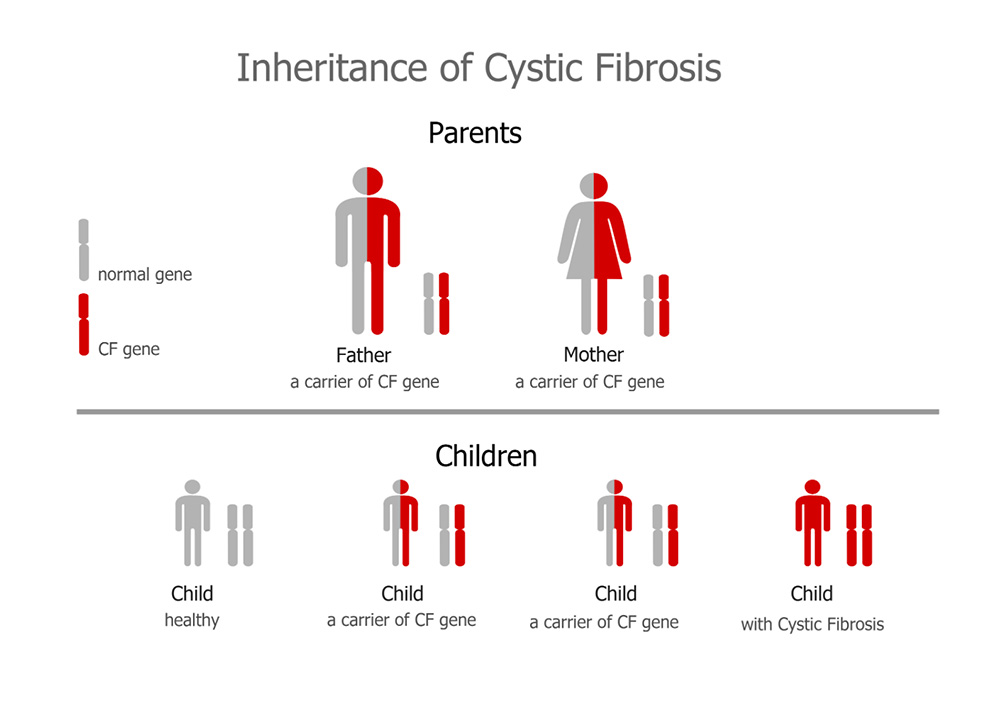
CF is an autosomal recessive genetic disorder. Both males and females can have CF or be carriers of the CF gene. If a person has only one copy of a CF gene, they are carriers of the CF gene. This person will not have CF. If a person has two copies of a CF gene, they will have CF.
If both parents carry a CF gene each (carriers) there is a 1 in 4 chance their child will be born with CF, and a 1 in 2 chance their child will be a carrier of the CF gene. This is the case for every pregnancy these parents have. If one parent has CF and one parent has two normal genes, then all of the children will be carriers.
Screening for CF is included in the newborn heel prick test. CF will be the diagnosis if there is a positive heel prick test, if a formal sweat test is positive for CF (the sweat test measures the amount of chloride in the baby’s sweat), and with a blood test to confirm the CF gene.
The common genetic mutation of CF is delta F508. Remember to have CF you need to have a CF gene from your mum, and a CF gene from your dad. They may be the same mutation (homozygous) or you may also have what is called a heterozygous combination which means you have two different mutations. New treatments (called CFTR modulator therapy) are available, and more are on the horizon. CFTR modulator therapy targets the CFTR protein and aims to change how it is working. Your CF mutation determines what is wrong with your CFTR protein so your medical team can work out which of the new medications may work for you.
Important things to note about CF incidence are:
- Males and females are affected equally
- Over 2000 different types of genetic mutations cause CF
In Australia and New Zealand, one in 25 people, or nearly one million in total, are carriers of the CF gene. Approximately one in every 3000 babies are born with CF, with a new diagnosis occurring approximately every 4 days.
